AUA 2026 Annual Meeting 2026 · Conference briefings
AUA 2026 — AI and Robots Are Both Here. They Haven't Met Yet.
We mined 3,200 abstracts (1,835 with fulltext, the remainder classified by title and session metadata) at the AUA 2026 Annual Meeting. 621 touch AI or robotic surgery — one in five. Single-port became the most-mined robotic subcategory, LLMs arrived with 51 abstracts and no consensus, and the intersection of AI and robotics barely exists. The tools are ready. The integration hasn't happened.

/ scale /
The scale
Six hundred twenty-one abstracts. That is the combined footprint of AI and robotic surgery at AUA 2026 — the union of 231 AI and 405 robotic papers, minus 15 that appear in both. For context, the entire meeting carries 3,200 abstracts (1,835 with fulltext, the remainder classified by title and session metadata) across all of urology. One in five papers this year touches a robot or an algorithm.
AUA now runs a dedicated AI session — IP04 — with 27 abstracts. That is a small but important administrative signal. It means the program committee decided AI is not a scattered curiosity that belongs inside other sessions. It is a category. Categories get budget, podium time, and repeat invitations. The same thing happened with robotic surgery a decade ago, and we know how that turned out.
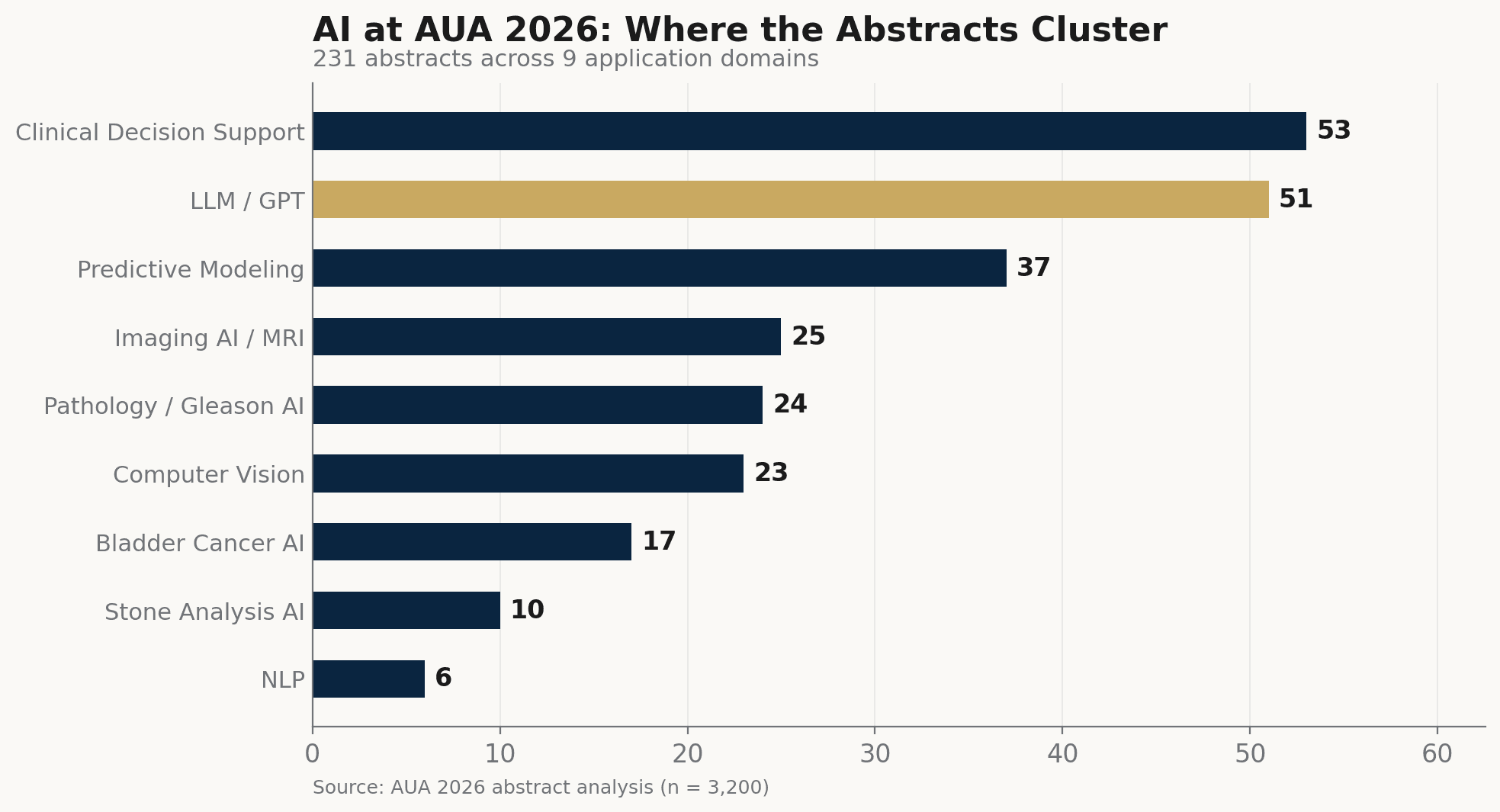
AI/ML abstract categories at AUA 2026. LLM/GPT studies (51) now form a distinct sub-field. Computer vision (23) and the strict AI-robot intersection (15) remain small.
Source: AUA 2026 program · AAI analysis
The distribution tells a second story. AI abstracts cluster in imaging, pathology, and clinical decision support. Robotic abstracts cluster in technique, outcomes, and platform comparison. The two clusters occupy different rooms in the same building. They share a convention center but not a research agenda. That separation is the structural observation this briefing will follow through its remaining sections.
/ robot-pivot /
The robot pivot: single-port rises
The most visible shift on the robotic surgery floor is not a new technique. It is a platform migration. Single-port robotic surgery produced 105 abstracts at this meeting, becoming the most-mined robotic subcategory — now appearing in more abstracts than robot-assisted radical prostatectomy (98), which has been the flagship procedure of urologic robotics for two decades. That said, single-port's clinical indications remain narrower and its learning curve steeper than multi-port systems. The crossover in abstract volume reflects a field that has moved past asking whether single-port works and is now asking how fast it scales.
The new entrants matter. Hugo RAS, Medtronic's robotic platform, appeared in 12 abstracts — an early signal, not yet an evidence base for procurement decisions, but the first meaningful body of clinical data from a serious da Vinci competitor. TOUMAI (MicroPort) contributes 5, Hinotori adds 2. None of these will displace Intuitive overnight. But the fact that three alternative platforms now generate peer-reviewed data at AUA changes the negotiating position of every hospital procurement committee in the room. Competition in surgical robotics has been theoretical for a decade. It is becoming empirical.
One ratio cuts deeper than any platform count. Across all 405 robotic surgery abstracts, outcomes studies outnumber technique descriptions by roughly two to one — 228 versus 135. (Abstract counts reflect volume of interest, not evidence quality.) A field that mostly publishes outcomes has passed its proof-of-concept phase. It is no longer arguing that robotic surgery can be done. It is measuring how well it performs at scale, across institutions, and across patient populations. That maturity marker is easy to miss in a program booklet. It is the most important number on the robotic floor.
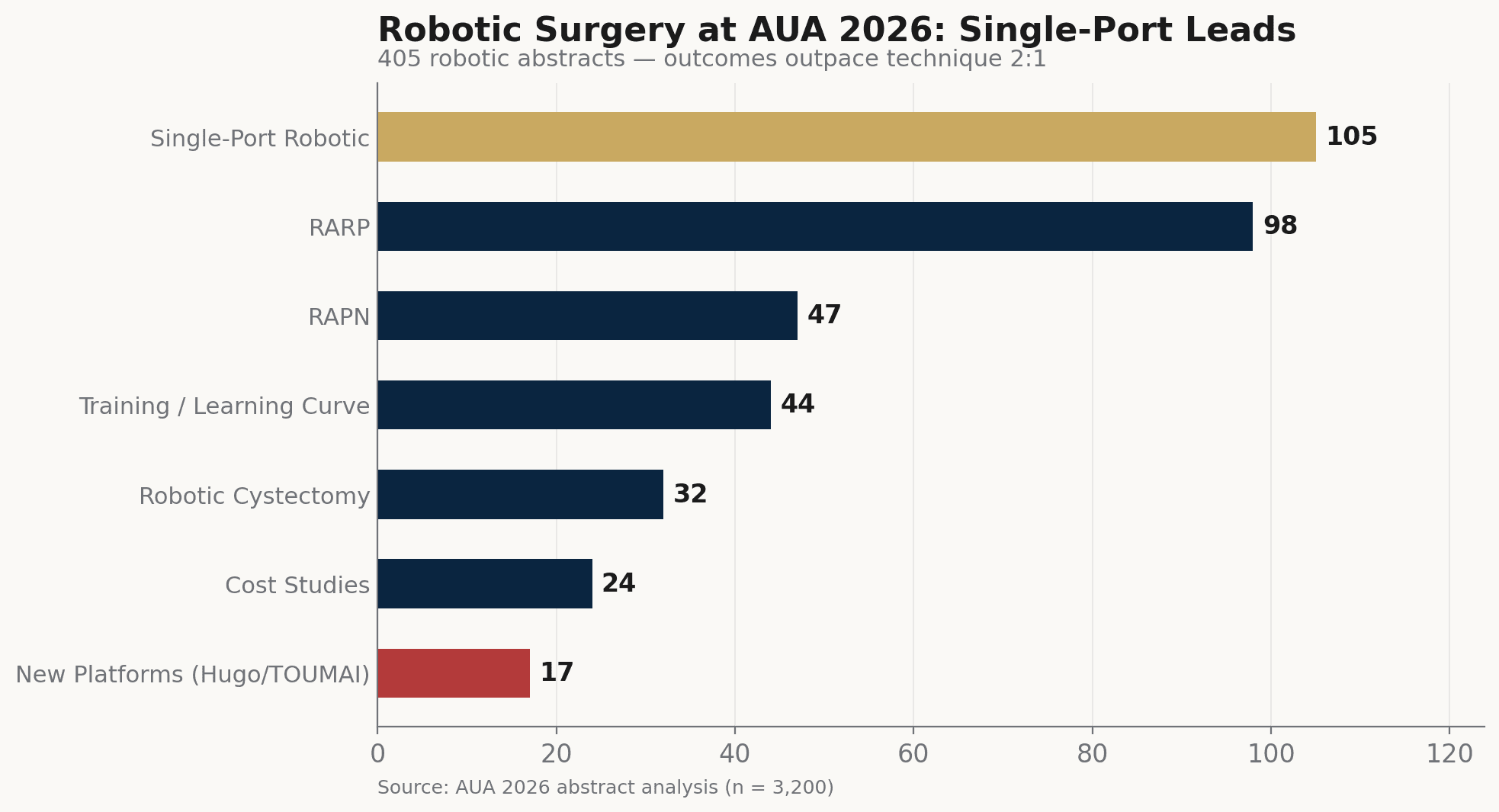
Robotic surgery sub-categories at AUA 2026. Single-port (105) became the most-mined robotic subcategory, now appearing in more abstracts than RARP (98) alone. Hugo RAS enters with 12 abstracts — an early signal.
Source: AUA 2026 program · AAI analysis
/ llm-invasion /
LLM arrival: 51 abstracts, zero consensus
Large language models arrived at AUA the way they arrive everywhere — fast, enthusiastic, and without a shared framework. Fifty-one abstracts mention GPT, LLM, or a named large language model. They span clinical decision support, pathology report interpretation, patient education material generation, surgical planning assistance, and bias detection in AI-generated recommendations. Most are single-center, proof-of-concept, or retrospective benchmarks. The breadth is impressive. The depth is not.
Most of these studies follow a recognizable pattern. Take a clinical question. Feed it to GPT-4 or a comparable model. Compare the output to expert consensus or guideline recommendations. Report concordance rates. A smaller but growing subset does the opposite — testing where LLMs fail, hallucinate, or reproduce existing biases in urologic care. These limitation studies are arguably more valuable than the concordance papers, because they map the boundaries of a tool rather than its best-case performance. But neither group has produced a validated clinical deployment. No abstract at this meeting reports an LLM integrated into a live clinical workflow with prospective outcome data.
That absence is not a failure. It is a timestamp. The field is in its question-asking phase, not its answer-shipping phase. Fifty-one abstracts say urology is paying attention to LLMs. Zero validated deployments say it has not yet figured out what to do with them. The gap between attention and implementation is where the next two years of work will happen — or won't.
/ ai-gap /
The gap where AI meets the robot
Here is the number that should bother everyone in both camps. Of the 231 AI abstracts and the 405 robotic surgery abstracts at this meeting, only 15 sit at the strict intersection — studies where AI methods and robotic surgery appear together, whether for outcome prediction, operative-note analysis, or surgical-phase recognition. Fifteen out of 621. That is 2.4 percent of the combined footprint. The most natural pairing in surgical technology — intelligent software guiding precision hardware — has almost no presence on this program floor.
Computer vision accounts for 23 abstracts total, and most of those involve diagnostic imaging rather than intraoperative surgical guidance. The training and learning curve literature is larger — 44 abstracts — and represents the most fertile ground for AI integration. Automated surgical skill assessment, phase recognition in recorded procedures, and predictive models for learning curve completion are all technically feasible today. A handful of abstracts explore them. But the standard training study at AUA 2026 still uses human proctors, subjective scoring, and retrospective case review. The AI tools exist. The training pipeline has not adopted them.
The pattern repeats across every robotic sub-specialty. Robotic partial nephrectomy (47 abstracts) could benefit from AI-assisted tumor segmentation and perfusion mapping. Robotic cystectomy (32 abstracts) could use automated lymph node identification. Single-port procedures — the fastest-growing category — could leverage real-time instrument tracking to compensate for reduced degrees of freedom. In each case, the computer science is published. The surgical application is not. This is not a technology gap. It is a workflow integration gap. Many algorithms show promising single-center results. The operating room has not made room for them.
/ takeaway /
What we take from Washington
AUA 2026 tells a story of two technologies growing up in the same house without talking to each other. Robotic surgery is mature — outcomes-driven, multi-platform, scaling past its flagship procedure as single-port became the most-mined subcategory. AI is arriving — 231 abstracts, a dedicated session, LLMs generating genuine research interest. But the intersection is nearly empty. Fifteen abstracts out of 621 is not a minor gap. It is a structural one.
The reason matters more than the number. Robotic surgeons publish about what they can measure with existing tools. AI researchers publish about what they can demonstrate on available datasets. Neither group has built the infrastructure to put an algorithm inside a live surgical workflow and measure what happens. The bottleneck is not algorithm performance — computer vision models for surgical phase recognition already achieve high accuracy in research settings. The bottleneck is workflow integration: data pipelines from the robot to the model, regulatory clearance for intraoperative AI, institutional review of real-time decision support, and surgeon trust in systems they did not train.
That integration layer — connecting validated AI tools to the surgical workflows that need them — is where the next phase of urologic innovation will be won or lost. AUA 2026 shows a specialty that is adopting both technologies in parallel. It also shows a specialty that has not yet asked itself the hard question: what does it take to make them work together? The tools are in the building. The wiring is not. That is the work ahead.