AACR Annual Meeting 2026 · Conference briefings
AACR 2026 — Reading the Phase 1 Floor
Phase 1 is where pharma puts its current bets in front of the field. We pulled all 442 first-in-human and Phase 1 abstracts at AACR 2026 to read what is being bet on this year — and how those bets are designed.
/ 01 /
The Phase 1 floor as a room
Of the 7,066 abstracts at AACR 2026, 442 carried first-in-human or Phase 1 framing — about 6% of the meeting. That share is steady year over year. What is up year over year is the share of explicitly dedicated Phase 1 sessions. Five abstract sessions were named for Phase 1 directly: "Phase I Clinical Trials in Progress" (28 abstracts), "Phase I and Phase II Clinical Trials in Progress" (28), "First-in-Human Phase I Clinical Trials" (23), "Phase 0 and First-in-Human Phase I Clinical Trials" (21), and "Phase I Clinical Trials" (20).
Together those five sessions ran 120 abstracts — roughly a third of all the FIH-flagged work at the meeting. The rest is distributed: about 80 in modality-specific sessions like ADC linker engineering and adoptive cell therapy; another 90 in target-specific sessions for tyrosine kinases, RAS inhibitors, and the like; and the remaining roughly 150 sit inside disease-track sessions, where Phase 1 design is treated as part of the disease story rather than a methodology of its own.
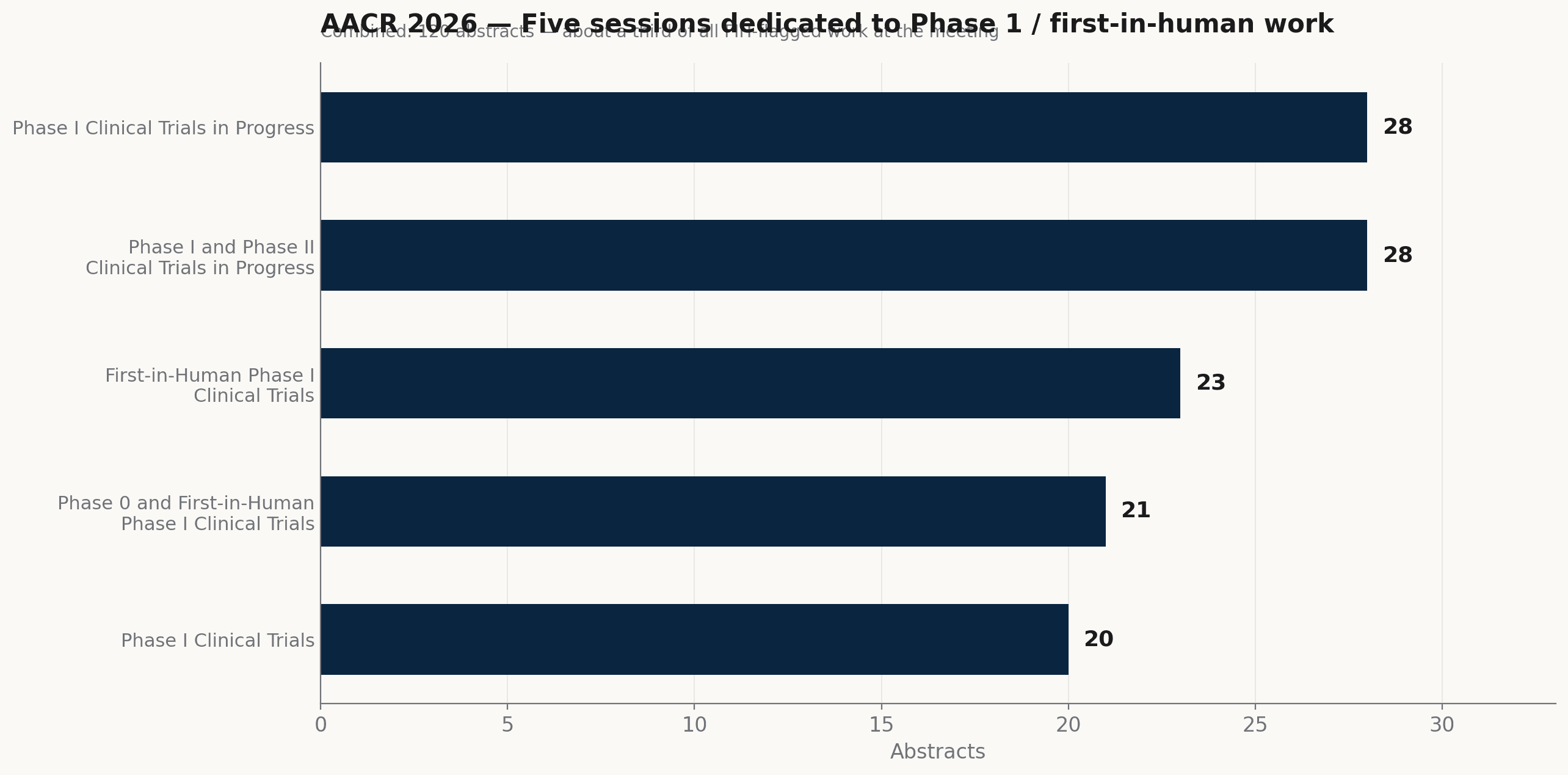
AACR 2026's five abstract sessions dedicated to Phase 1 / first-in-human work. Together they hosted 120 abstracts — roughly a third of all FIH-flagged work at the meeting.
Source: AACR 2026 program · AAI analysis
Read together, this says the meeting is treating Phase 1 in two ways at once. It is its own discipline — there are dedicated rooms for it. And it is content that travels with the rest of the program. That dual citizenship is healthy: trial methodology and disease biology are being talked about in the same rooms, not in parallel ones.
/ 02 /
Two modalities run the room
When we tagged the 442 FIH abstracts by modality, two led by a wide margin. Antibody-drug conjugates show up on 79 abstracts. Bispecific T-cell engagers and other bispecific antibody constructs show up on 62. The two tags overlap in places — bispecific ADCs sit inside both buckets — so by combined tag count those modalities cover roughly 141 abstract entries, somewhere close to a third of the Phase 1 floor (the unique count is a little lower).
The two waves share a common move. Both turn a target into a delivery problem. ADCs use the antibody as a homing device for a chemical payload, with the linker chemistry, internalization biology, and bystander effect all shaping where and when the payload kills. Bispecifics use the antibody as a homing device most often for a T cell, sometimes for an NK cell, sometimes for a second tumor-side target. Both buy potency by combining specificity with execution, and both buy clinical risk that the field is still learning to manage — payload toxicity and ocular signals for ADCs, cytokine release and on-target/off-tumor effects for bispecifics. The technology is mature enough to enter Phase 1 in volume. The safety stories are not yet settled.
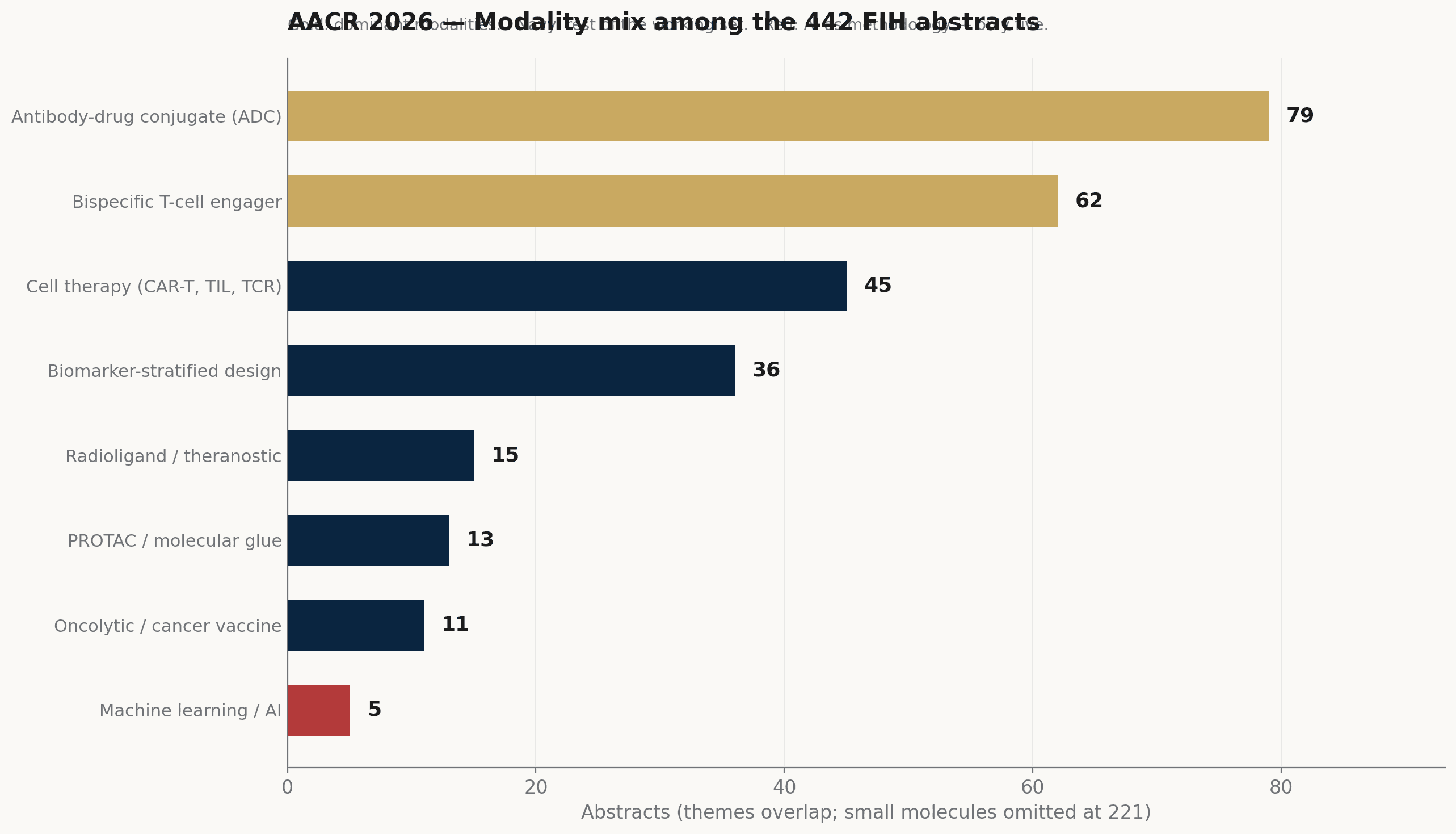
Modality mix among the 442 FIH abstracts at AACR 2026 (excluding the broader "small molecule" bucket, which carries 221). ADCs and bispecific T-cell engagers dominate; AI as methodology is conspicuously small at five.
Source: AACR 2026 program · AAI analysis (themes overlap)
Cell therapies — CAR-T, TIL, TCR-engineered T cells — added another 45 abstracts. Quieter on the floor than ADCs and bispecifics, but the trajectory is steady: more solid-tumor entries, more allogeneic platforms, a few first-in-human protocols moving from heme into glioblastoma, hepatocellular, and prostate. Targeted protein degraders — PROTACs and molecular glues — carried 13 first-in-human abstracts. Small in absolute number, but visible: three years ago that count was effectively zero.
/ 03 /
Where the trials actually run
The Phase 1 floor is concentrated, not spread. We tallied institutional affiliations across the FIH abstracts and the same dozen sites kept appearing.
Memorial Sloan Kettering Cancer Center is on roughly one in ten FIH abstracts. UT MD Anderson Cancer Center is close behind. Dana-Farber Cancer Institute, Massachusetts General, and Mayo Clinic round out the academic top tier. Sarah Cannon Research Institute — a network of affiliated dedicated Phase 1 units rather than a single site — appears on 13 abstracts. As an industry-trial affiliation it remains the most concentrated single Phase 1 network in the United States.
On the sponsor side, the recurring names are familiar: AstraZeneca, Johnson & Johnson, Roche/Genentech, Bristol Myers Squibb, Pfizer. What is more visible than in past years is how often Asia-headquartered pharma — Daiichi Sankyo, Innovent, BeiGene — appears as the lead sponsor on FIH abstracts in solid tumors. The trend is clear enough in this year's program to be worth naming, even if the long-run trajectory is still being charted.
Concentration like this is operationally efficient. Sites that run twenty Phase 1 protocols a year build muscle the rest of the field cannot replicate quickly. But the ecosystem is also fragile in a real way. A few institutions and a few sponsors carry most of the load, and the gap to the second tier is wide. Any biotech that wants to start an FIH trial outside the dozen-or-so centers that dominate this list is looking at a steeper operational learning curve than the published timelines suggest.
/ 04 /
The design layer is finally moving
The most interesting shift this year was not in what gets tested. It was in how the trials are designed. 36 of the 442 FIH abstracts named biomarker-stratified design as a core feature: patient selection by tumor genomics, by immunohistochemistry, by ctDNA fraction, or by PSMA-style imaging-determined eligibility.
That is about 8% of the FIH floor. Compared with the same tagging applied to AACR programs five years ago — closer to 2% — that is a real move, though program-language tagging across years is imprecise enough that the magnitude is best read as a hypothesis the next year of protocol filings will confirm or refute, rather than a settled longitudinal benchmark. The direction of travel is clear, though. Biomarker-driven Phase 1 trials used to be built only when a target was so molecularly tight that stratification was unavoidable. Now, in protocols whose targets carry any biomarker correlate at all — PSMA-anchored prostate trials, KRAS-G12 selected lung trials, MSI-high tumor-agnostic baskets — stratified design reads more like an expected register than the exception it was.
What has not reached the floor yet is the next step: model-based dose finding (Bayesian, EWOC, BLRM with overdose control), AI-assisted basket selection, and adaptive design with real-time biomarker readout. The 3+3 escalation rule is no longer the unquestioned default — it is still common, particularly in academic-led protocols — and the field is openly experimenting with model-based alternatives. What has not yet happened is adoption at scale. That is where the next year of design progress will likely show up. It is also the layer where AI methodology should be entering soonest.
/ 05 /
What we take, including what is still missing
AACR 2026's Phase 1 floor reads like a field that has matured operationally. The modalities are clear, the sites that run them are well organized, and the design layer is finally moving. The work is concentrated, sometimes uncomfortably so, but it ships. That is what operational maturity looks like.
One number stood out the same way it did in our last two briefings. Of the 442 FIH abstracts, only five named machine learning, deep learning, or AI as a methodology. Five. In a meeting where ML is the ninth most common keyword overall, the layer of work that decides which patients enter early trials, what doses they get, and how toxicity signals are read is still mostly classical. The infrastructure exists. The translation has not happened in early oncology trials.
Closing that gap is, plainly, what Apex AI Institute's drug-development line was set up to do. Pillar 1 builds AI-augmented FIH scout systems and computational landscapes for early oncology trials — exactly inside the design layer that this year's meeting confirmed is moving but not yet AI-native. The next briefing in this series will go deeper into one piece of that work. The same template that carried this article will carry that one.