AACR Annual Meeting 2026 · Conference briefings
AACR 2026 — How Prostate Cancer Research Moved This Year
We pulled the 295 prostate-cancer abstracts out of AACR 2026 to ask one practical question: where is the field actually moving — and what is still surprisingly small?
/ 01 /
The size of the prostate room
Of the 7,066 abstracts published at AACR 2026, 295 touched prostate cancer either by primary topic, keyword, or session title. That is about 4% of everything at the meeting. By keyword frequency, prostate cancer ranked eighth among solid tumors — behind breast (453), pancreatic (296), and colorectal (275), and ahead of gastric and head-and-neck cancers.
The prostate work is spread, not concentrated. The most prostate-loaded sessions this year were not single-organ blocks. They were cross-cutting topics: "Novel Strategies to Reverse Drug Resistance" carried six prostate-flagged abstracts, "Circulating Tumor Cells, Metastasis, and Dissemination Biology 1" carried six, and "Genetic Epidemiology 1: GxE, GWAS, Polygenic Risk Scores, and Post-GWAS" carried six. Prostate cancer at AACR rarely gets its own room. It travels through the rooms about resistance, biomarkers, and translational pharmacology.
Sessions hosting the most prostate-cancer-flagged abstracts at AACR 2026. The work is mostly traveling through cross-cutting sessions on resistance, dissemination, and translational pharmacology rather than dedicated single-organ blocks.
Source: AACR 2026 program · AAI analysis
That dispersion is itself the most informative number. It says the field is not trying to define a new disease subtype this year. It is trying to retool the same molecule — androgen-driven cancer — across imaging, drug delivery, blood-based monitoring, and access to care. So that is where the rest of the briefing goes.
/ 02 /
The androgen receptor is still the protagonist
Across the 295 abstracts, 44 named the androgen receptor or castration-resistance directly. That is roughly 15% of the prostate work — by far the largest internal cluster. The recurring frame was the same: how do we keep turning the AR off, or make it irrelevant, after the standard hormonal therapies have stopped working?
The angles split four ways. Targeted-degrader chemistry — PROTACs and related approaches — showed up in roughly nine abstracts, betting that you can solve resistance by removing the protein, not just blocking it. Hormone-receptor-signaling sessions added another five, focused on alternative AR splice variants and downstream cofactors. A separate cluster used chromatin and metabolic biology to reframe resistance as an epigenomic state rather than a single mutation. And a smaller group sat at the antibody-drug conjugate intersection, using AR-pathway biology to direct payload.
What is interesting is not any single mechanism. It is that the program treats castration-resistant prostate cancer as a chronic problem with multiple right answers in parallel — degrader chemistry, splice-variant targeting, epigenetic resetting, metabolic vulnerability — rather than a single therapeutic frontier. The community has stopped looking for the next single drug class and started running several at once.
/ 03 /
PSMA has become the connective tissue
Fourteen abstracts named PSMA directly. Add radiopharmaceutical and theranostic platforms (12 abstracts), and PSMA-adjacent imaging work (about 9 more), and you have roughly 35 abstracts where PSMA is the molecule the work hangs on. It is doing the most non-AR connective work in prostate research right now.
The reach is the surprise. PSMA used to mean PET imaging and 177Lu-PSMA radioligand therapy — a tight diagnostics-and-therapy pair. This year you can see it stretching: PSMA-targeting bispecific T-cell engagers, PSMA-conjugated antibody-drug conjugates, theranostic pairings with new isotopes, and even non-prostate trials using PSMA imaging to select patients in liver and other indications. The molecule has become a delivery handle, not just a target.
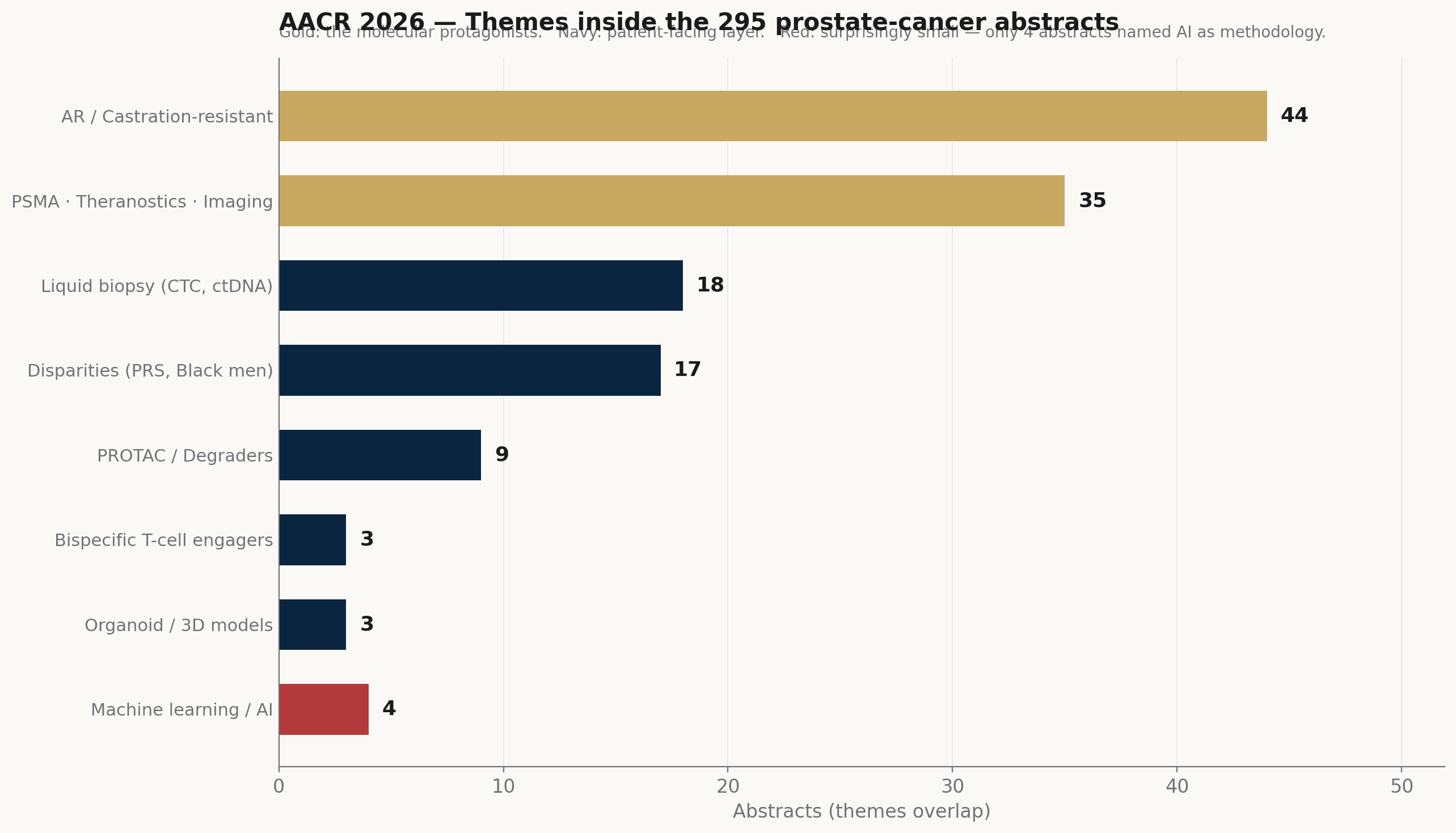
Internal theme distribution across the 295 prostate-cancer abstracts at AACR 2026. The two molecular protagonists (AR/CRPC and PSMA-anchored work) carry the most volume; liquid biopsy and disparities form the patient-facing layer; AI is the conspicuous outlier on the small side.
Source: AACR 2026 program · AAI analysis (themes overlap)
For early-trial design, that matters. A target that crosses imaging, immunotherapy, and radioligand classes is one where biomarker-stratified first-in-human design has the best chance of working. PSMA is the rare prostate-cancer asset where the imaging readout, the patient-selection biomarker, and the therapeutic mechanism can all be the same molecule. Watch this space — the convergence is recent.
/ 04 /
Reading the patient, not the molecule
Two clusters of work look outward from the cell to the patient. Together they account for roughly 35 abstracts, and they share one move: shifting the question from "what is the cancer made of?" to "what does the cancer look like in a person, over time?"
Liquid biopsy carries 18 abstracts — the largest sub-area outside AR and PSMA. Circulating tumor cells, ctDNA, cell-free RNA, miRNA panels. The framing has shifted in a quiet but real way. A year or two ago the questions were about feasibility — can we detect prostate cancer in blood? This year the questions are about timing — can we use what is in blood to time the next treatment change, predict resistance before it shows up on imaging, or stratify patients before a trial begins? That is the move from possibility to operational tool.
Seventeen abstracts engaged disparities — racial differences in incidence and outcome, polygenic risk scores recalibrated for non-European ancestry, the iCCaRE consortium's virtual-reality decision-support work for Black men at the point of diagnosis. The methodological sharpness is noticeably up year over year. Polygenic risk scores are being recalibrated rather than reused; access-to-care is being studied as a measurable variable, not a footnote. This is one of the few corners at AACR 2026 where prostate cancer gets a dedicated session room of its own.
/ 05 /
What we take, including what is still small
Read together, AACR 2026 says prostate-cancer research has stabilized into a multi-front game around two molecules — AR and PSMA — with the patient-facing layer (liquid biopsy, disparities) catching up. The progress is real, and it is incremental rather than disruptive. That is not a complaint. Cancer research that is settling into operational maturity is research that ships.
One number stood out as surprising. Of the 295 prostate-cancer abstracts, only four directly named machine learning, deep learning, or artificial intelligence as the methodology. Given that AI was the ninth most common keyword across the whole meeting — ahead of metastasis and drug resistance — that is a striking under-representation in this disease. The infrastructure is here. The clinical translation in prostate cancer has not yet caught it.
That gap is exactly where Apex AI Institute's drug-development line works. Pillar 1 builds AI-augmented first-in-human scout systems and computational landscapes for early oncology trials, with prostate cancer among the indications we have on file. The next briefing in this series will go deeper into one piece of that work. The same template carries this article and will carry that one.