ASCO Annual Meeting 2026 · Conference briefings
Genitourinary Cancer at ASCO 2026: The Prostate, Bladder, and Kidney Studies
The 2026 ASCO program carried 481 genitourinary cancer abstracts. This briefing summarizes the prostate, bladder, and kidney studies that reported full results — organized by cancer, each with its trial, size, and main numbers, and with data tables reproducing the key figures.
/ overview /
The genitourinary program in numbers
Of the abstracts carrying a genitourinary subtrack tag, 481 fell into the three major cancers and their rarer neighbors. The studies below are the ones with mature or otherwise notable results in each disease.
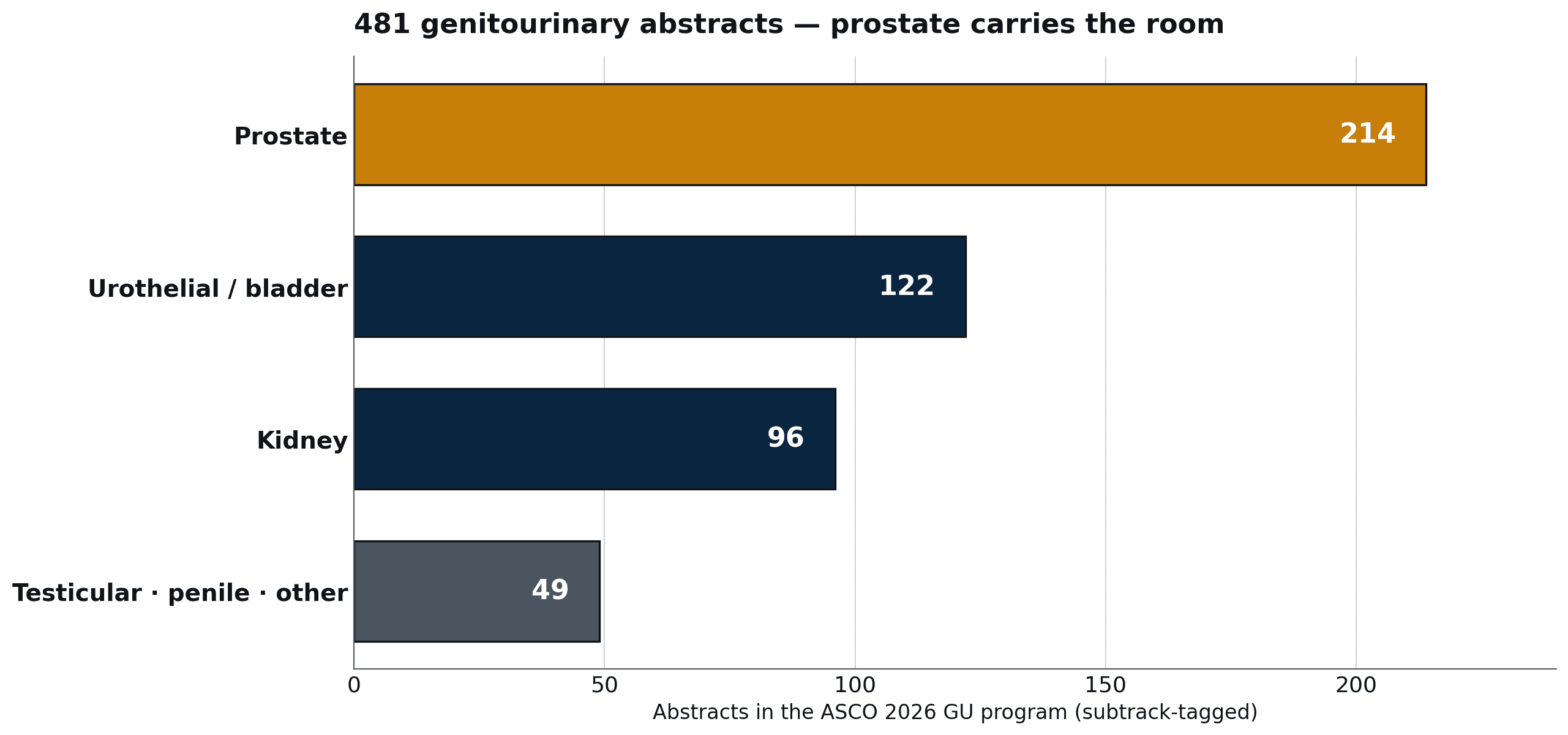
The 481 genitourinary abstracts in the ASCO 2026 program, by cancer.
Source: ASCO 2026 public program · AAI subtrack analysis
Prostate cancer carried the largest share, with about 214 abstracts across localized, hormone-sensitive, and castration-resistant disease. Urothelial and bladder cancer followed with about 122, kidney cancer with 96, and testicular, penile, and other histologies made up the rest.
/ prostate-intensify /
Prostate cancer: moving treatment earlier, and adding a PARP inhibitor
Two studies tested moving treatment usually given in late disease into earlier, hormone-sensitive disease; one tested adding a PARP inhibitor in first-line castration-resistant disease.
PSMAddition is a phase 3 trial of the radioligand 177Lu-PSMA-617 — a radioactive drug aimed at the prostate-specific membrane antigen (PSMA) — added to androgen-deprivation therapy plus an androgen-receptor pathway inhibitor in metastatic hormone-sensitive prostate cancer. Across 1,144 patients it improved radiographic progression-free survival, with a hazard ratio of 0.72 (95% CI 0.58–0.90), and delayed the time to castration resistance (hazard ratio 0.70). Point estimates were similar across disease-volume and de novo/recurrent subgroups, though several subgroup confidence intervals were wide. Patients had to have PSMA-positive disease on a PET scan to enter.
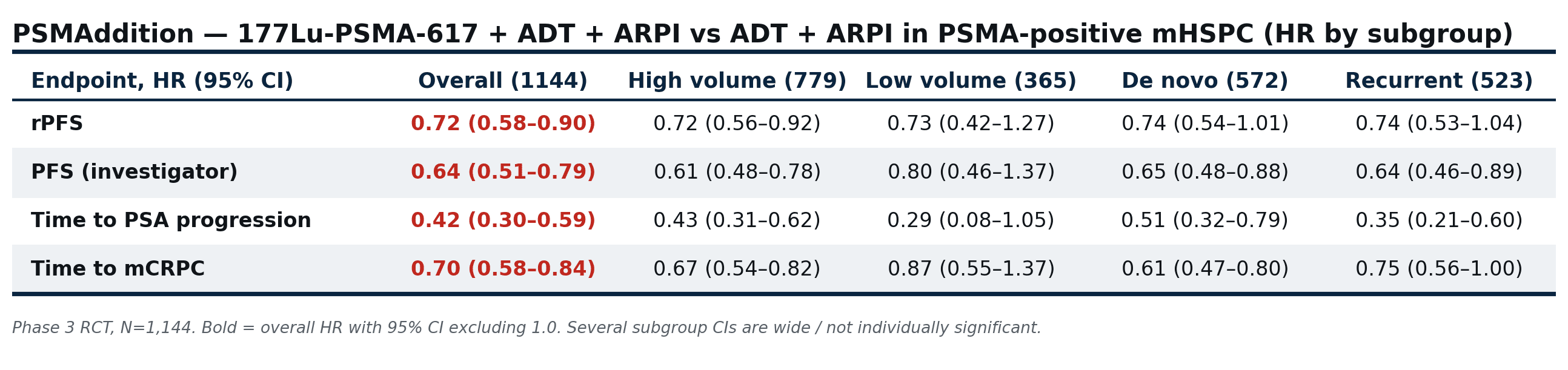
PSMAddition: hazard ratios for 177Lu-PSMA-617 added to standard therapy, overall and by subgroup.
Source: released ASCO 2026 abstract (PSMAddition, phase 3)
AcTION is a phase 1 dose-escalation study of an alpha-emitting radioligand, 225Ac-PSMA-617, in 101 men with metastatic castration-resistant prostate cancer. In men with no prior chemotherapy or androgen-receptor inhibitor, the PSA-50 response rate was 85%; in men who had already progressed after the beta-emitter 177Lu-PSMA, it was 52.5%. There were no dose-limiting toxicities, and the most common side effect was grade 1–2 dry mouth (over 90%).
FUZUPRO is a phase 3 trial that added the PARP inhibitor fuzuloparib to abiraterone in 496 men with first-line metastatic castration-resistant prostate cancer. Overall radiographic progression-free survival improved (hazard ratio 0.71). The effect was larger in the DNA-repair-defective subgroup (hazard ratio 0.51; median 27.7 vs 13.9 months) than in the repair-intact group (hazard ratio 0.81). Overall survival was immature, and grade 3 or higher anemia occurred in about 20%.
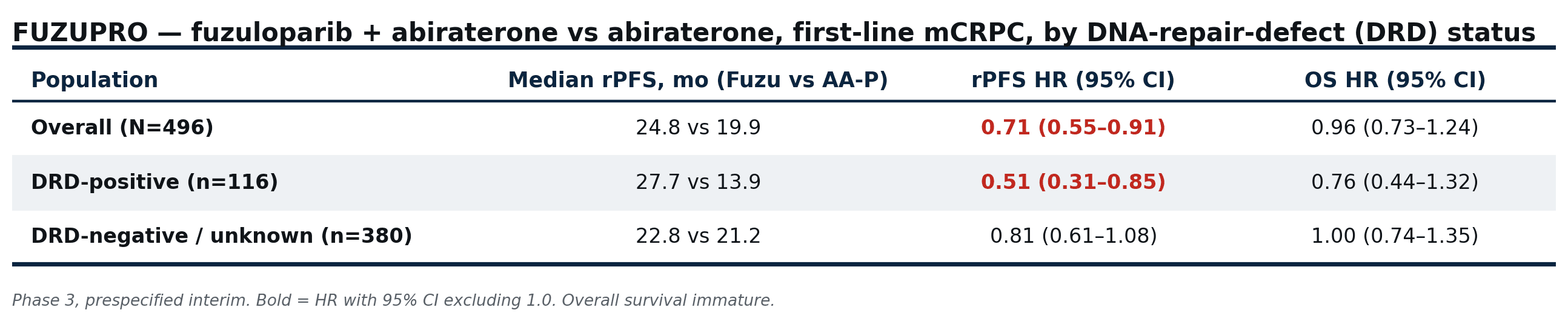
FUZUPRO: progression-free and overall survival with fuzuloparib added to abiraterone, by DNA-repair status.
Source: released ASCO 2026 abstract (FUZUPRO, phase 3 interim)
/ prostate-personalize /
Prostate cancer: stopping, switching, and selecting chemotherapy
Three studies addressed when treatment can stop, which androgen-receptor inhibitor to choose, and who needs added chemotherapy.
A-DREAM is a single-arm phase 2 trial in 78 men with metastatic hormone-sensitive prostate cancer who had reached a PSA below 0.2 ng/mL on testosterone suppression plus an androgen-receptor inhibitor. Treatment was stopped entirely. At 18 months, 41% were both treatment-free and had recovered testosterone; among those who resumed, one progressed in a way that required a switch.
ARACOG is a randomized phase 2 trial comparing two androgen-receptor inhibitors on cognition in 111 men. At 24 weeks, the most-affected cognitive domain declined 36.1% on enzalutamide versus 15.8% on darolutamide (p=0.009). Every patient who crossed over did so from enzalutamide to darolutamide, none in the other direction.
An analysis of the ENZAMET trial (1,125 men) tested whether the Decipher genomic classifier predicts benefit from adding docetaxel. Among men on androgen-deprivation plus enzalutamide, a high Decipher score (above 0.85) was associated with worse five-year survival (adjusted hazard ratio 2.29); when docetaxel was added, that difference disappeared (hazard ratio 1.08). Low-score men showed no clear benefit from added docetaxel.
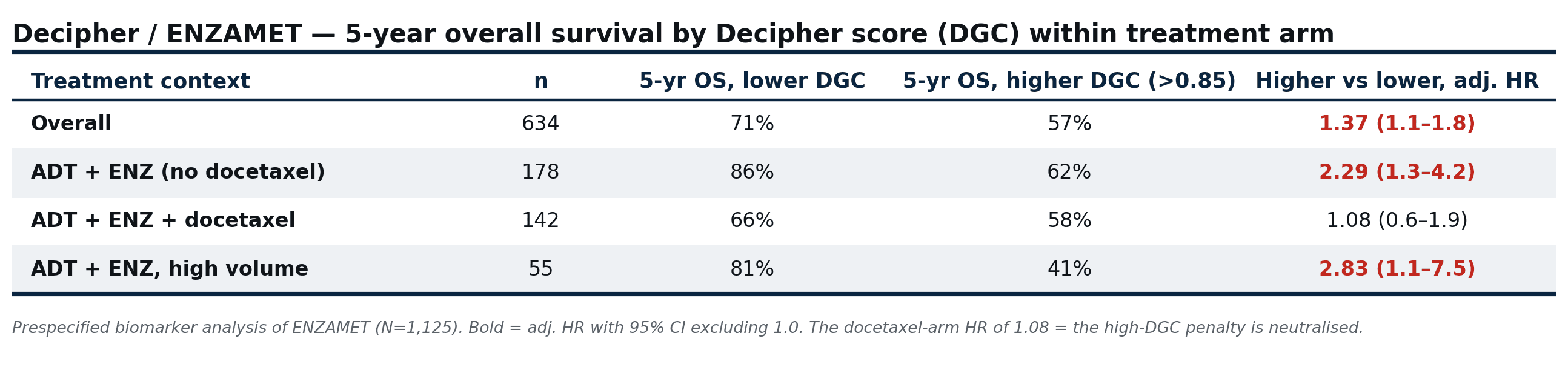
Decipher/ENZAMET: five-year overall survival by genomic score, within each treatment arm.
Source: released ASCO 2026 abstract (Decipher analysis of ENZAMET)
/ urothelial /
Urothelial cancer: a new first-line standard
The first-line standard in advanced urothelial cancer has shifted from platinum chemotherapy to enfortumab vedotin plus pembrolizumab (EV+P), an antibody-drug conjugate aimed at nectin-4 combined with an immune-checkpoint inhibitor.
EV-302 reported 3.5-year follow-up (median 42.8 months). Median overall survival was 33.6 months with EV+P versus 15.9 months with chemotherapy (hazard ratio 0.53). Among patients who reached a complete response, two-thirds did so after first having a partial response, converting over a median of five further cycles.
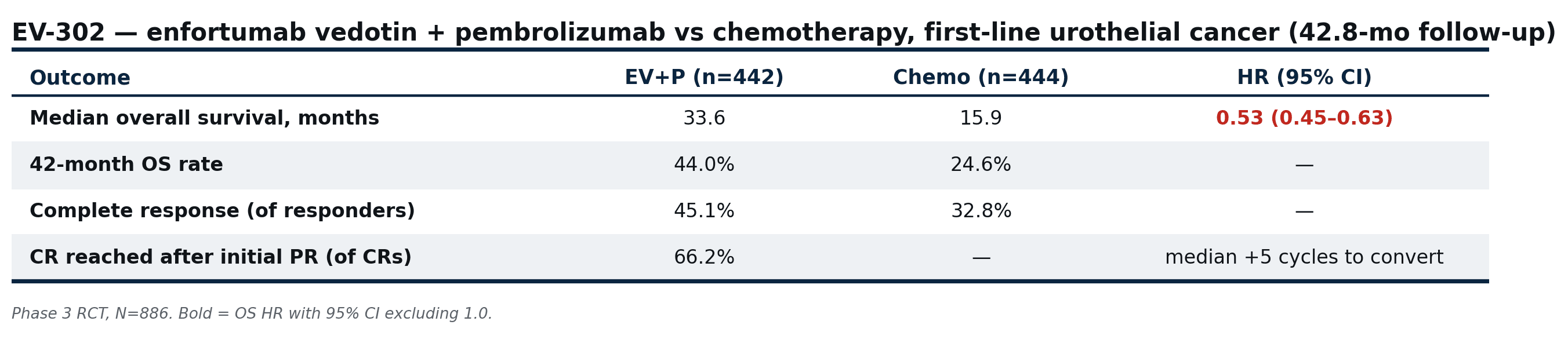
EV-302: outcomes with enfortumab vedotin plus pembrolizumab versus chemotherapy, first-line urothelial cancer.
Source: released ASCO 2026 abstract (EV-302, phase 3)
MAIN-CAV tested adding cabozantinib to avelumab maintenance after platinum chemotherapy. It closed early — 68 of a planned 654 patients — after EV+P became the preferred first-line standard. Adding cabozantinib showed no survival benefit (hazard ratio 1.41) and raised grade 3 or higher toxicity from 24% to 39%.
An early-phase study (phase 1b/2) of the next nectin-4 antibody-drug conjugate, bulumtatug fuvedotin plus toripalimab, reported an 83% response rate in 47 patients, including activity in patients unfit for cisplatin. A phase 3 trial is ongoing.
/ bladder /
Muscle-invasive bladder cancer: treatment around surgery
In muscle-invasive bladder cancer, several studies addressed treatment around surgery and the option of preserving the bladder.
SAKK 06/19 is a single-arm phase 2 trial that added intravesical recombinant BCG to perioperative chemotherapy plus immunotherapy in cisplatin-eligible muscle-invasive disease. The pathologic complete response rate was 65% among the 40 patients who underwent surgery (55% across all 47 enrolled). The trial paired perioperative therapy with cystectomy.
RAD-IO added durvalumab to chemoradiation in muscle-invasive bladder cancer, a bladder-preserving approach. In a single-arm, evaluable cohort, the preliminary one-year disease-free survival was 79%.
The AMBASSADOR trial previously showed that adjuvant pembrolizumab after surgery extended disease-free survival from 14.2 to 29.6 months. The quality-of-life analysis reported here found no significant difference between pembrolizumab and observation on any measure.
/ kidney /
Kidney cancer: selecting adjuvant therapy, and non-clear-cell histology
A circulating-tumor-DNA (ctDNA) analysis from the KEYNOTE-564 trial (994 patients) tested whether a blood test for tumor DNA could identify which patients need adjuvant immunotherapy after kidney-cancer surgery, since most patients never recur. The test was specific (96–99%) but its sensitivity was only 10–15%, so it missed most patients who later recurred. It is not yet usable as a selection tool.
A single-arm phase 2 trial of cabozantinib plus nivolumab in non-clear-cell kidney cancer reported an overall response rate of 43%, ranging from 88% in fumarate-hydratase-deficient tumors to 0% in chromophobe disease — on small subgroups (eight and seven patients respectively). Non-clear-cell kidney cancer behaves differently by histologic subtype.
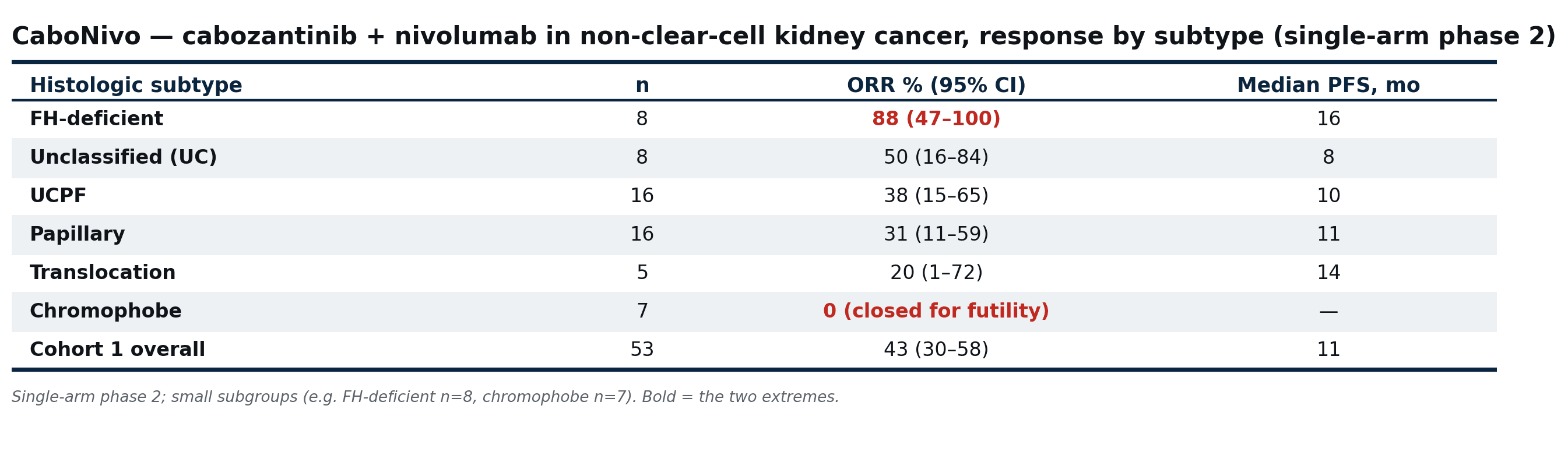
CaboNivo: response to cabozantinib plus nivolumab in non-clear-cell kidney cancer, by histologic subtype.
Source: released ASCO 2026 abstract (CaboNivo, single-arm phase 2)
Across prostate, bladder, and kidney cancer, the studies at ASCO 2026 combine new agents with new ways to decide who should receive them — a target on a PET scan, a DNA-repair test, a genomic score, a histologic subtype. Apex AI Institute's Pillar 1 builds AI methods for that second part — patient selection and biomarker reading in early oncology trials — held to external validation.