AUA Annual Meeting 2026 · Conference briefings
AUA 2026 in Metastatic Prostate Cancer: Five Trends, from the Triplet Intensification Gradient to PSMA-PET Stage Migration
Five live arguments inside the 50 advanced and metastatic prostate-cancer abstracts at AUA 2026: where each patient lands on the triplet intensification gradient, PSMA-PET reclassifying nmHSPC into metastatic disease, PSMAddition's PSA sub-analysis on a positive rPFS readout, survivorship and access becoming a real section, and the sequencing / biomarker / AI gap that the meeting did not close.
/ 01 /
Size of the advanced-PC room at an AUA meeting
Of the 3,200 abstracts at AUA 2026, 463 touched prostate cancer by primary topic, keyword, or session. Fifty of those sit in the Advanced / Metastatic track — roughly 11% of the prostate work, and about 1.5% of the meeting as a whole. The work clusters in three backbone sessions: IP38 (Advanced I), IP73 (Advanced III), and PD23 (Plenary Discussion). The rest scatter across Global Gateway posters and a handful of cross-cutting sessions.
Setting distribution is the second thing to mark. mCRPC carries 19 abstracts, mHSPC carries 18, nmCRPC drops to 5, oligometastatic 3, biochemical recurrence 3. Hormone-sensitive and castration-resistant disease now read almost as twins at this meeting, a shift from a few years ago when mCRPC was the loudest room. nmCRPC keeps shrinking partly because PSMA-PET reclassifies those patients into the metastatic column, a point we return to in section 03.
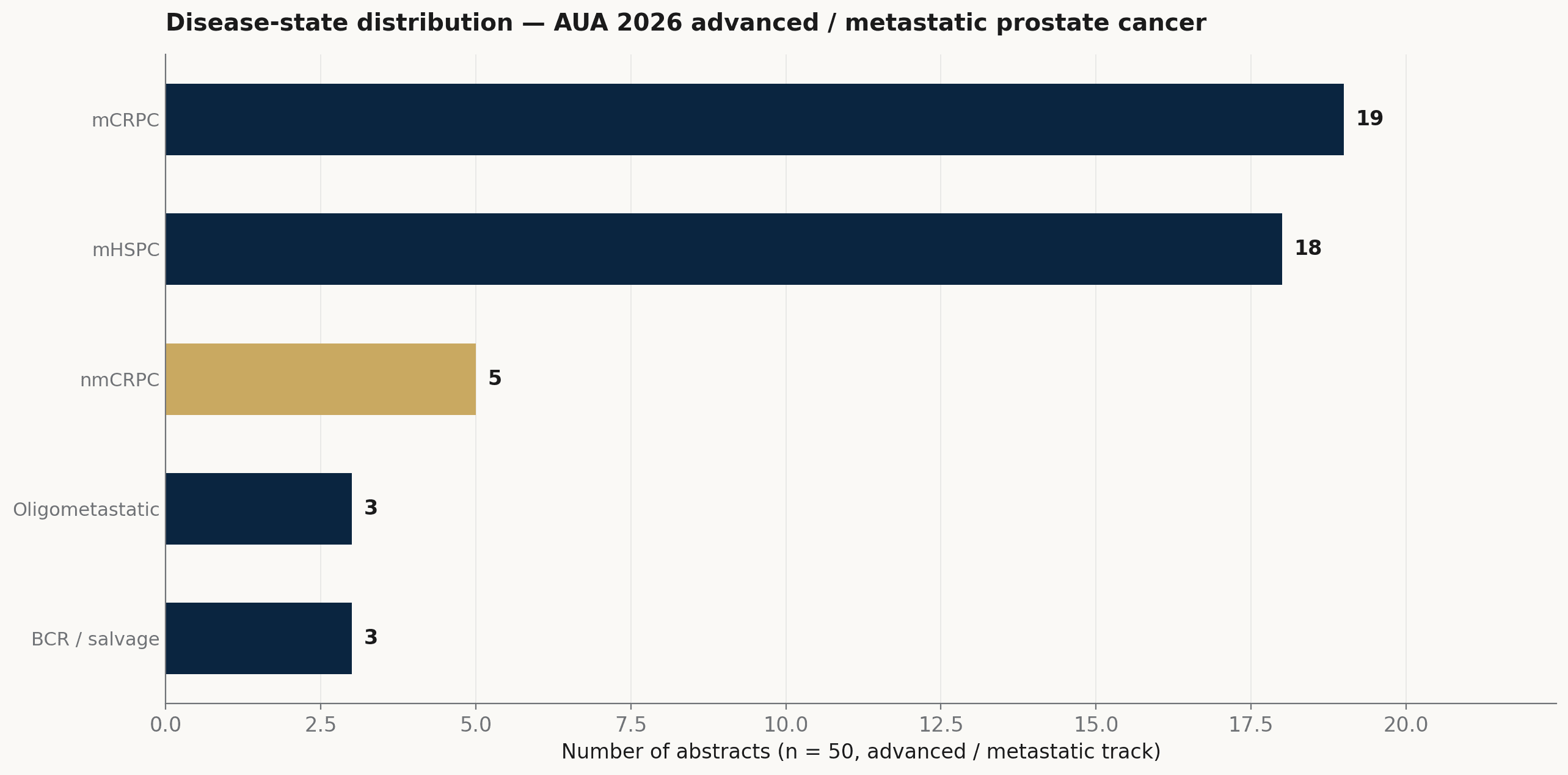
Disease-state distribution across the 50 advanced and metastatic prostate-cancer abstracts at AUA 2026. mHSPC and mCRPC now sit almost evenly weighted; nmCRPC has shrunk as PSMA-PET reclassifies patients out of the non-metastatic column.
Source: AUA 2026 program · AAI analysis
Real-world abstracts outnumber randomized trials twenty to thirteen. That ratio itself is the take. AUA is not GU ASCO; this audience does not ask whether the next phase 3 readout reaches statistical significance. It asks why the prescription that already carries a hazard ratio does not show up in the clinic. That framing carries through the rest of the briefing.
/ 02 /
The intensification gradient is the mHSPC argument
The loudest question in mHSPC at AUA 2026 is not whether triplet therapy (ADT + an androgen-receptor pathway inhibitor + docetaxel) works. It is where each patient lands on an intensification gradient — castration alone, ARPI doublet, or triplet — and which lever (case-mix, referral path, urologist judgment, cost) actually moves them. Six abstracts engage triplet directly; another fifteen sit in the doublet / triplet real-world envelope around them.
Dr. Paolo Zaurito of IRCCS San Raffaele Hospital (Milan) presented Sweden's NPCR population registry analysis (Abstract IP38-12): 3-year overall survival in de novo mCSPC rose from 51% (95% CI 49–52%) in the 2016–2018 baseline cohort as ARPI doublet and docetaxel triplet adoption climbed in subsequent years. Dr. Soichiro Yoshida's Bayesian individual-patient-data reanalysis (Abstract IP38-13) delivers the read the field has been waiting for. The investigators concluded that 'ADT + ARAT doublet remains the rational default; triplet therapy may be considered selectively in high-volume patients' — a finer-grained answer than the original RCTs gave, and one that pushes back against uniform triplet application. Dr. Lixin Hua's prospective high-volume mHSPC multimodal series (Abstract IP38-08) sits alongside.
Behind the trial-level data sits the practice-pattern layer specific to AUA. Dr. Kasey Berscheid (University of Toronto, Abstract IP73-14) measured urologist-level variation in ADT intensification in a universal-health-care cohort: the variance partition coefficient attributable to physician ran only 4.6% overall, rising modestly to 7.8–8.5% in 2020–2022, with most variation driven by patient characteristics. That corrects the easy story that 'urologists vary wildly.' Dr. Neal Shore of START Carolinas / Carolina Urologic Research Center (Abstract IP38-10) mapped urology-to-oncology referral patterns in metastatic disease: median time from diagnosis to oncology referral was not reached in a meaningful subgroup, meaning many patients still sit in the urology lane longer than guideline-default narratives assume. Together they describe an intensification gradient anchored on patient case-mix, not a clean doublet-versus-triplet binary.
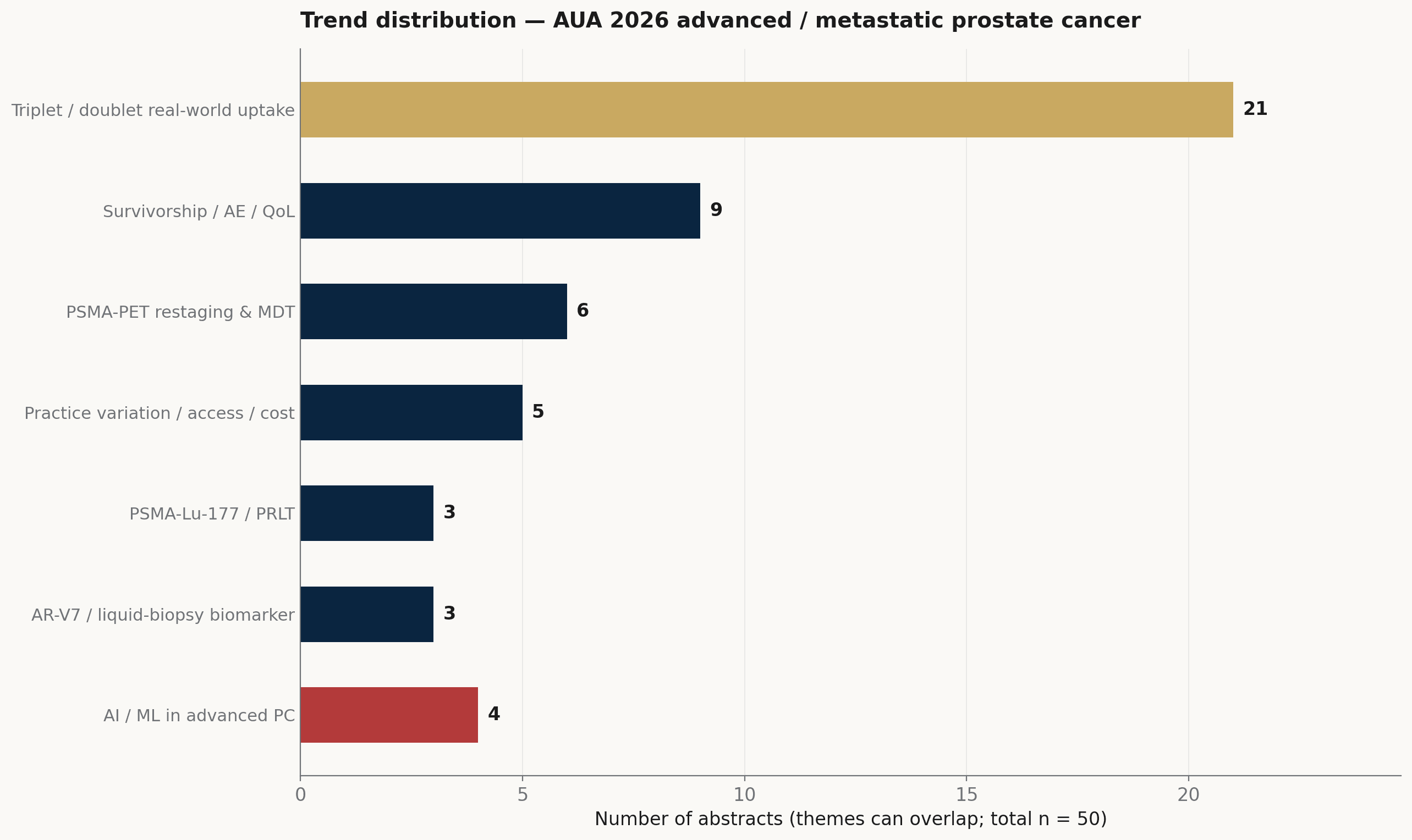
Trend distribution across the 50 advanced / metastatic abstracts at AUA 2026. The triplet-uptake real-world cluster carries the most volume; PSMA-PET restaging and survivorship/AE work form the next two layers; AI/ML in advanced PC stands out on the small side.
Source: AUA 2026 program · AAI analysis (themes overlap)
/ 03 /
PSMA-PET stage migration has outpaced the treatment evidence
PSMA-PET has been quietly running ahead of the trials. Stage migration — the Will Rogers effect in the imaging age — keeps reclassifying patients out of the non-metastatic and into the low-volume metastatic column, and the clinical question is no longer 'is the patient metastatic?' but 'now that imaging says they are, do we operate, irradiate, or sequence?' At least six abstracts at AUA 2026 sit on that question along the earlier boundaries: biochemical recurrence, oligometastatic mCSPC, de novo mHSPC, and the post-systemic primary. Caveat: this is not yet a mCRPC local-therapy revolution. mCRPC remains a systemic problem in this program. What is moving is the line between non-metastatic and low-volume metastatic — and what to do once a patient crosses it.
Dr. Alessandro Viti (IRCCS San Raffaele, Abstract IP73-18) gave the cleanest example: take patients who would have qualified for EMBARK on conventional imaging, restage them with PSMA-PET, and a meaningful share reclassify into the metastatic column. The trials that defined nmHSPC may have been treating a population whose underlying disease state nobody could see. Dr. Lei Xu (Abstract PD23-09) brought cytoreductive radical prostatectomy back to the table in oligometastatic mCSPC during the Plenary Discussion session, reporting oncological outcomes for surgery + hormonal therapy in a setting where systemic-only used to be the unquestioned answer. Dr. Samuel Morris of Imperial College London (Abstract IP73-20, n=81, ADT + docetaxel up-front in de novo mHSPC) looked the other direction: pathological complete response or minimal residual disease in the primary occurred in 26.3%. A quarter of treated primaries effectively clear on systemic therapy alone, which directly shapes how to select candidates for cytoreductive surgery. Dr. Anna Jansen of the Netherlands Cancer Institute (Abstract IP73-30) wired PSMA-PET into salvage whole-pelvis radiotherapy for post-RP biochemical recurrence: only 4.6% of patients had in-field recurrence at the 5-year mark, most relapses were close out-of-field nodal, and grade 3–4 toxicity ran 8% acute / 29% late. Promising biochemical PFS with manageable toxicity.
PSMA-Lu-177 itself carries only three abstracts here, which understates its weight. PSMAddition's radiographic-PFS primary endpoint already read out positive in mid-2025; Dr. Fred Saad of the University of Montreal Hospital Center presented the PSA-endpoint sub-analysis at AUA 2026 (Abstract PD23-02) from that phase 3 trial of [177Lu]Lu-PSMA-617 plus an ARPI in mCSPC, with Novartis disclosing a 58% lower risk of PSA progression (hazard ratio 0.42) on 2026-05-17. The next watch points are not whether PSMAddition will read out — that has happened — but OS maturity, regulatory action in mCSPC, and how the field sequences PRLT against doublet and triplet ARPI regimens. Dr. Eman Ahmed's Mayo Clinic cohort (Abstract IP73-16) quietly counters the easy story by asking how to actually image disease progression after Lu-177: 11C-choline PET/CT detected radiographic progression more frequently and at lower PSA levels than PSMA PET/CT in post-Lu-177 patients. A reminder that PSMA-PET is not automatically the right surveillance tool once you have therapeutically saturated PSMA expression.
/ 04 /
Two persistence layers urology owns: toxicity, then money
Nine of the 50 abstracts — roughly 18% — engage the long-tail layer where urologists actually do the day-to-day work long after the medical oncologist has set the regimen. The work splits cleanly into two: toxicity persistence (anemia, febrile neutropenia, older-patient tolerance, ARPI cross-class switching) and financial persistence (reduced-dose dosing, orchiectomy's quiet return). Both layers are growing because patients are now living long enough on therapy to make them matter.
Dr. Neal Shore (returning, this time on Abstract IP73-04: TALA + ENZA in mCRPC, n=398) measured anemia's bite on quality of life: 45% of patients required dose modification for anemia and 164 hit grade 3–4; patient-reported global health, physical functioning, and fatigue all declined in the assessments before anemia clinically presented, then improved after transfusion or dose modification. Anemia was a quality-of-life event well before it became a lab abnormality. Dr. Shunsuke Tazawa of Hirosaki University (Abstract IP73-02, n=214, ARPI-based triplet in mHSPC) found grade 3-or-higher febrile neutropenia in 13% of patients overall, and bone-modifying agents (zoledronic acid / denosumab) significantly reduced that risk on multivariable analysis. A cheap protective intervention with previously unappreciated bone-marrow benefit. Dr. Masaki Kyono of Kobe University (Abstract IP38-06) walked docetaxel in CRPC: of 487 patients, 162 (33%) were aged ≥75, and PSA50 (47% vs 42%, p=0.27), median PFS (8.0 vs 6.0 months, p=0.11), and median CSS (46 vs 40 months, p=0.09) were all statistically similar between older and younger. Older patients tolerate full-dose docetaxel with comparable efficacy, contrary to the implicit caution baked into many practice patterns. Dr. Yoichiro Tohi of Kagawa University (Abstract IP73-08) looked at switching ARPI after apalutamide discontinuation for rash (17/117 patients switched, 40% of rashes were grade ≥3): PFS and OS showed no difference between switch and non-switch groups in both mCSPC (p=0.55) and nmCRPC (p=0.67). Switching within the ARPI class after rash does not visibly cost the patient outcome.
The access and cost thread is the other half of this layer. Dr. Ryuma Tanaka (Hirosaki University, Abstract IP73-09) named a question very few medical-oncology meetings would touch: can a reduced-dose ARPI maintain efficacy in nmCRPC and save the patient meaningful money? The analysis projects substantive cost savings without efficacy loss, although the data are early. Dr. Darryl Mitteldorf of Malecare Cancer Support — a patient-advocacy organization, not an academic center — mined patient-and-care-partner online forum threads on advanced PC (Abstract IP38-28): orchiectomy appeared in 64.5% of analyzed threads, abiraterone in 49.7%, enzalutamide in 33.4%, degarelix in 33.4%, relugolix in 33.0%. Orchiectomy is not the retired option the ARPI era assumed; cost, adherence, and end-of-injection burden are the recurring patient-voiced reasons it comes back. That a patient-advocacy group is the source of this signal — not an academic urology department — is itself the take. This is the section where AUA sounds like AUA and not like an oncology meeting downstream of it.
/ 05 /
Three gaps the meeting did not close: sequencing, biomarker, access
Read together, AUA 2026 says advanced prostate cancer has split into a guideline-adoption problem on the front end and a persistence problem on the back end, with PSMA imaging as the connective tissue running through both. The mHSPC question has moved from whether triplet is better to where each patient sits on the intensification gradient. The mCRPC question is no longer whether systemic therapy is the only answer. Both moves are quiet, both are recent, and both are visible in the program.
Three gaps the meeting did not close are worth naming, in order of clinical weight. First: sequencing logic. With doublet, triplet, post-progression ARPI cycling, PSMA radioligand therapy, taxane re-treatment, and PARP inhibitors all live, the field now has more lines than a typical mCRPC patient will reach — yet the program offered almost no head-to-head sequencing data. Second: biomarker-guided selection. AR-V7 and ctDNA appear at the edges in only a handful of abstracts; the AUA pool does not yet treat liquid biopsy as a routine selector, which is the precondition for picking the right line at the right time. Third: access and equity scale-up — the reduced-dose ARPI and orchiectomy work in section 04 is the right instinct, but it is small. Worth noting in passing: bipolar androgen therapy appears in zero abstracts (Sam Denmeade's program has not pushed into the AUA pool), immunotherapy (checkpoint inhibitors, sipuleucel-T) likewise zero (the immune-cold consensus has not loosened at AUA), and AI as methodology runs fewer than five abstracts in this track — a structural under-representation given how much AI lift the three gaps above would actually take.
Apex AI Institute's drug-development line sits inside those last gaps. Pillar 1 builds first-in-human scout systems and computational landscapes for early oncology trials, with advanced and metastatic prostate cancer among the indications on file; the AI work that matters here is sequencing logic and biomarker-guided selection, not surgical-AI analogues. The next briefing in this series will read the focal-therapy room, which is the second-largest unmined layer of the prostate track at AUA 2026.