AACR Annual Meeting 2026 · Conference briefings
AACR 2026 — Head and Neck Cancer Gets a New Pipeline
We pulled 358 HNSCC abstracts from AACR 2026 to read what changed this year: architecturally novel drugs, diversifying biomarkers, and three distinct bets against checkpoint-refractory disease — arriving all at once.
/ 01 /
The size of the head-and-neck room
Of the 7,070 abstracts at AACR 2026, 358 carried head-and-neck or HNSCC framing — about 5% of the meeting. By keyword volume, head and neck ranked behind breast, lung, colorectal, and pancreatic, but ahead of gastric and bladder. It is a mid-size disease track — large enough to read structurally, small enough that individual abstracts are still distinguishable.
The work does not cluster in dedicated head-and-neck sessions. Like prostate cancer at this meeting, HNSCC disperses through cross-cutting sessions: drug resistance, immunotherapy combinations, ADC linker engineering, biomarker-based patient selection. Head and neck at AACR rarely gets its own room — it travels through rooms about the technologies being applied to it. That pattern itself is information: the field is being pulled forward by platform technologies, not by disease-specific biology alone.
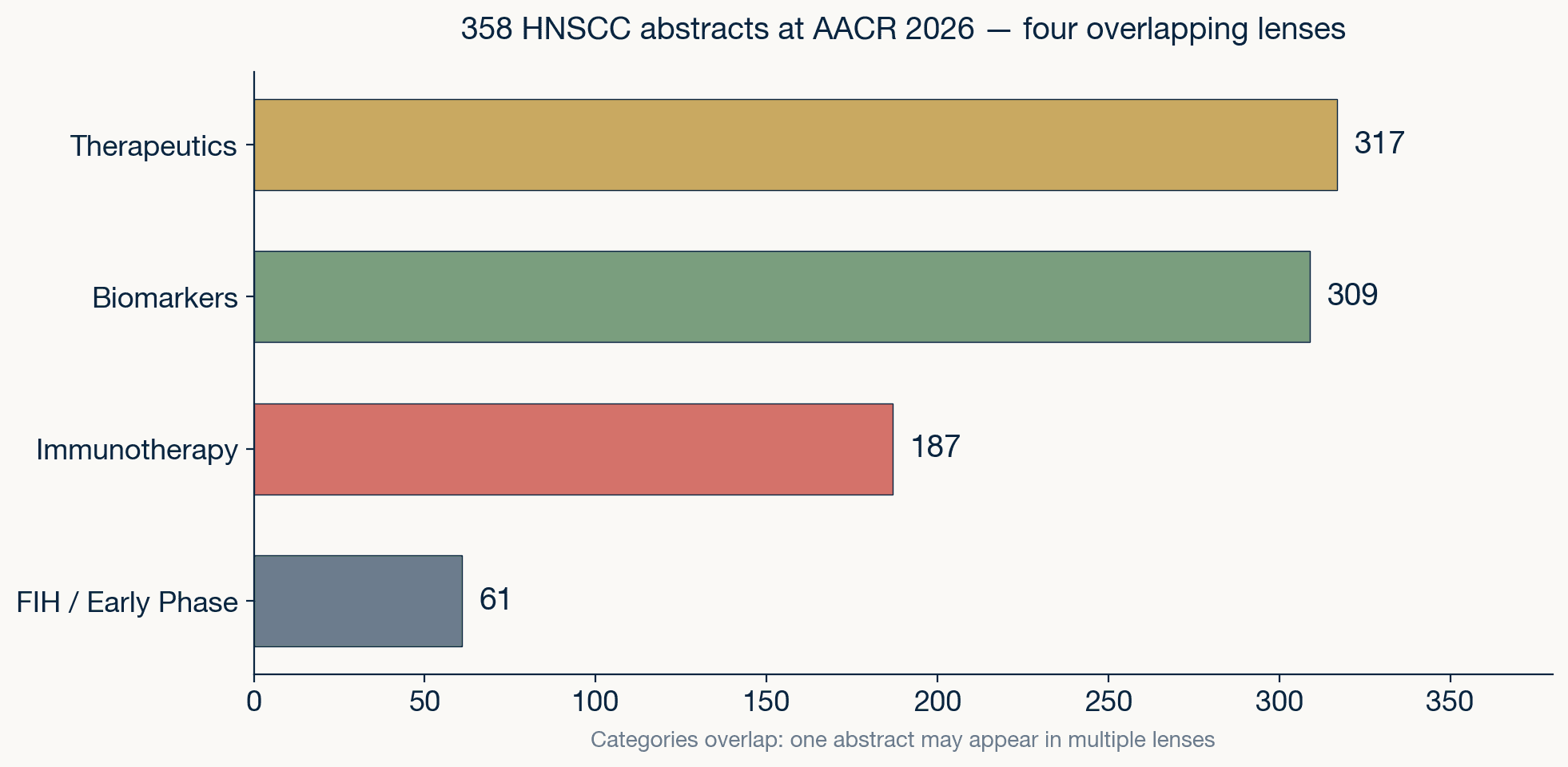
HNSCC abstract composition at AACR 2026. Categories overlap: one abstract may appear in multiple lenses. The therapeutics fraction (88.5%) is unusually high for a disease track at this meeting.
Source: AACR 2026 program · AAI analysis
The 317-of-358 therapeutics fraction is striking. Almost nine in ten HNSCC abstracts at this meeting involve a drug, a target, or a combination. This is a disease track that has shifted from biology-first to therapeutics-first in its AACR footprint — a change that would have been hard to imagine five years ago, when the head-and-neck floor was dominated by HPV epidemiology and immune-microenvironment characterization.
/ 02 /
The new molecules are not iterations
The drugs arriving on the HNSCC floor at AACR 2026 are not refinements of existing classes. They are architecturally new molecules, many first-in-class, designed against targets the field did not have delivery solutions for until this year. The common design move: engineering specificity at a level that was not technically feasible two or three years ago.
Six ADC programs stand out. STRO-227 targets PTK7 with a dual-payload design — two distinct cytotoxic agents on one antibody, a format still rare anywhere in the clinical pipeline. RT023 is a first-in-class CEACAM5/EGFR bispecific ADC: the antibody itself is bispecific before the payload is attached, giving it two tumor-side anchors where cetuximab had one. OBI-904 uses a Globo H glycan-targeting approach to Nectin-4, designed specifically to overcome enfortumab vedotin resistance — a second-generation molecule engineered against the resistance pattern of an existing drug. PF-08046033 (Pfizer) targets GPNMB, a marker enriched in mesenchymal-shifted tumors. CS5006 targets integrin β4, a basal-layer adhesion molecule novel as an ADC target in HNSCC. NEOK001 (ABL206) is a B7-H3×ROR1 bispecific ADC with dual-target coverage.
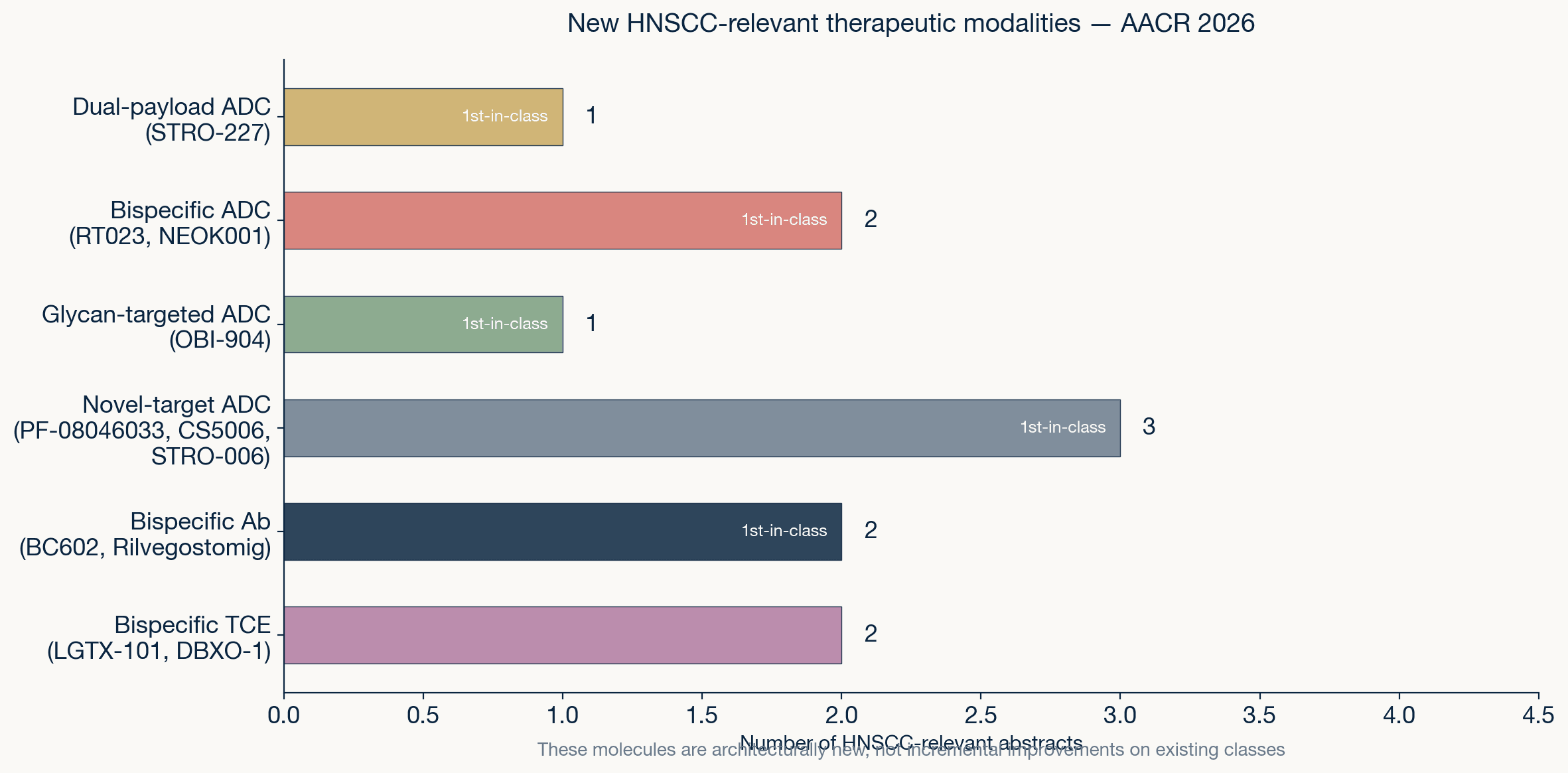
New HNSCC-relevant therapeutic modalities at AACR 2026. Most are first-in-class — the pipeline is architecturally novel, not incremental.
Source: AACR 2026 program · AAI analysis
On the T-cell engagement side, LGTX-101 is a Nectin-4×CD3 bispecific T-cell engager whose binding architecture was derived using machine learning — an actual AI-to-clinic pipeline, not a retrospective analysis. DBXO-1 targets multiple peptide-MHC complexes simultaneously, a design that tries to cover tumor heterogeneity at the immune-recognition level. BC602 is an LGR5×EGFR bispecific antibody at IND-enabling stage with HNSCC as a planned indication (IND filing expected Q3 2026). And rilvegostomig (AZD2936), a PD-1/TIGIT bispecific, showed 28.6% immune activation rate in HNSCC patient-derived tumor explants versus 9.5% for anti-PD-1 monotherapy — with the highest responses in oral cavity samples.
One mechanistic abstract reframes the EGFR resistance problem for the entire field. IL-1α expression was shown to induce drug resistance to all generations of EGFR inhibitors in HNSCC — first through fourth generation, including non-covalent and degrader formats. The implication: EGFR-TKI failure in HNSCC is not a problem that next-generation TKIs will solve on their own. It is an inflammatory microenvironment problem, and the fix points toward anti-IL-1 combination strategies rather than better EGFR binders.
/ 03 /
Beating checkpoint-refractory: three distinct bets
The checkpoint-refractory problem is the central clinical challenge in HNSCC. Only about 20% of patients respond to immune checkpoint blockade. In HPV-negative disease — the harder subgroup, with 14 abstracts at this meeting focused specifically on it — even the recent KEYNOTE-689 trial showed limited response to PD-1 blockade. AACR 2026 reveals at least three mechanistically distinct strategies being pursued in parallel, which is new. Historically, the answer was "add another checkpoint."
The first bet is bispecific checkpoint redesign. Rilvegostomig combines PD-1 and TIGIT blockade in a single molecule, and the preclinical evidence — including a head-to-head comparison against anti-PD-1 in HNSCC patient-derived explants — suggests the format outperforms sequential monotherapy. Separately, single-cell spatial profiling of HPV-negative HNSCC now shows why anti-PD-1 alone falls short: tumor-reactive T cells infiltrate malignant islands but are driven into deep exhaustion by chronic antigen stimulation, while CXCL14-mediated chemotactic recruitment is insufficient to replenish them. The bispecific format is an engineering response to a biological reality that single-agent checkpoint therapy cannot overcome.
The second bet abandons the systemic checkpoint framework entirely. Intratumoral IL-12 in combination with HDAC inhibition was shown to overcome checkpoint-refractory tumors by reprogramming the local microenvironment — converting immunologically cold tumors into hot ones without relying on systemic T-cell activation. This is a fundamentally different philosophy: instead of releasing the brake on existing T cells, it rebuilds the engine locally.
The third bet uses ADCs not just as cytotoxic delivery vehicles but as immune primers. Several of the ADCs in the previous section — STRO-227, RT023 — are designed with payloads or mechanisms that trigger immunogenic cell death, effectively using the ADC to re-prime an immune response that checkpoint therapy failed to activate. The three bets are not competing for the same patient. They are competing for different failure modes of checkpoint therapy. The field has stopped asking "did checkpoint fail?" and started asking "why did it fail in this patient?"
/ 04 /
The measurement layer is diversifying
For a decade, HPV status — practically, p16 immunohistochemistry — was the only clinically actionable biomarker in HNSCC. At AACR 2026, at least five distinct biomarker modalities are entering clinical validation, and they measure fundamentally different things. The common move: measuring the tumor in motion, not what it is but what it is about to do.
The PECAN trial reported interim results on tumor-informed ctDNA detection in HNSCC — the liquid biopsy arm graduating from feasibility to clinical utility for recurrence monitoring. More striking: genome-wide cell-free DNA fragmentomes were shown to enable early detection of HNSCC from both blood and saliva. The saliva angle is unique to head and neck — no other solid tumor has a non-invasive body fluid that directly bathes the primary tumor site. A parallel study demonstrated a microfluidic platform for label-free capture of p16-positive circulating tumor cells in oropharyngeal cancer, taking the HPV biomarker from tissue to blood with an engineering solution.
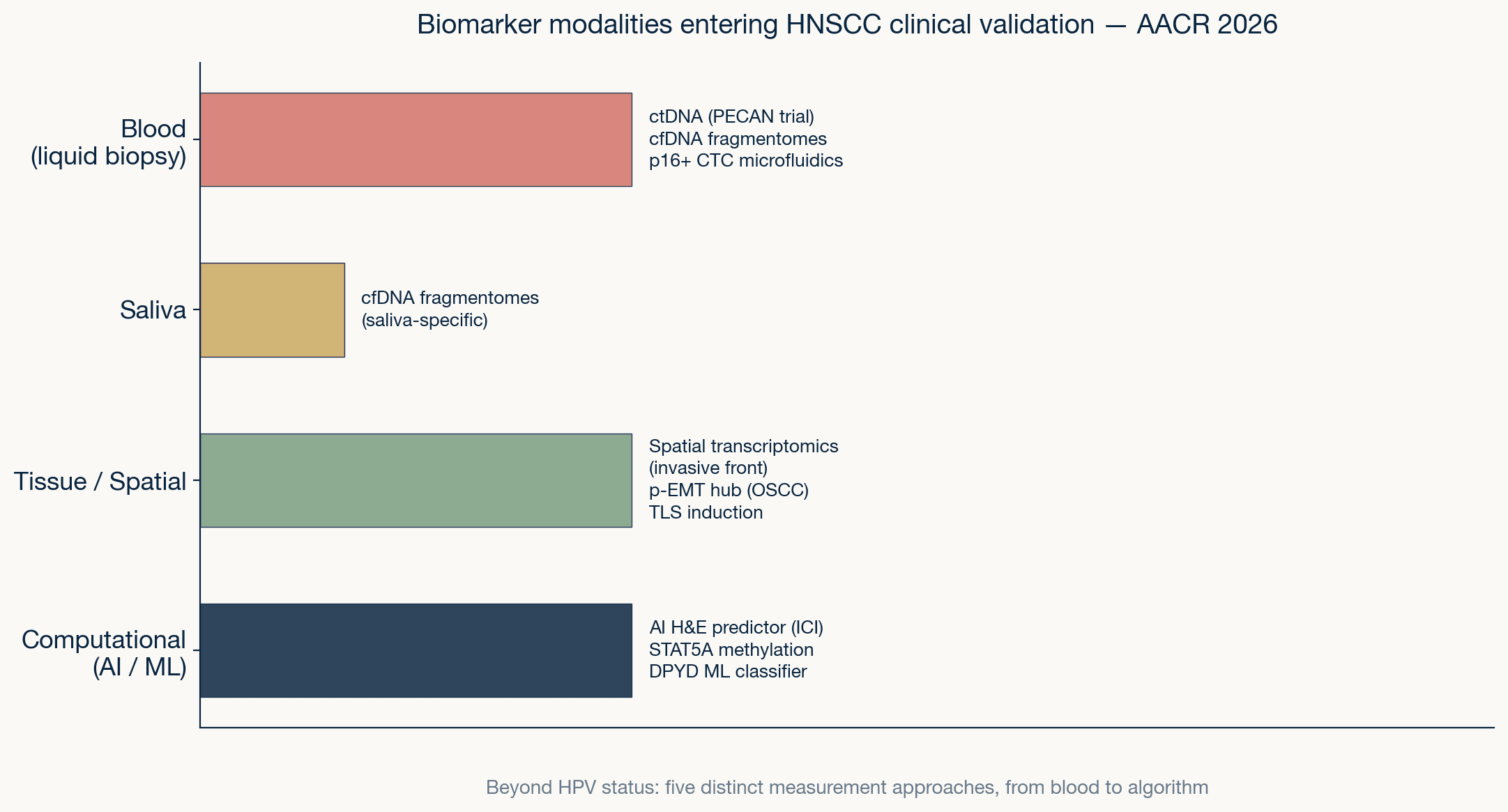
Five biomarker modalities entering HNSCC clinical validation at AACR 2026, organized by source: blood, saliva, tissue/spatial, and computational.
Source: AACR 2026 program · AAI analysis
On the tissue and computational side, spatial gene expression profiling at the invasive front was shown to predict aggressive CTC release and early recurrence in oral squamous cell carcinoma. The partial epithelial-to-mesenchymal transition (p-EMT) hub — a spatially defined cell-state niche with its associated DC2-macrophage ecosystem — was identified as a recurrence predictor in OSCC. And an AI-derived histopathology score, calculated directly from standard H&E slides, was validated as a predictive marker for checkpoint inhibitor response in advanced HNSCC — outperforming CPS in preliminary comparisons. The biomarker layer is no longer waiting for a single test to replace HPV status. It is branching into multiple measurement modalities, each reading a different dimension of the tumor's trajectory.
/ 05 /
What we take, including what has not arrived yet
AACR 2026 says HNSCC is no longer the therapeutic backwater it was five years ago. The pipeline is architecturally novel — dual-payload ADCs, glycan-targeted conjugates, ML-derived T-cell engagers — rather than incremental. The biomarker layer is diversifying past HPV into ctDNA, salivary fragmentomes, spatial transcriptomics, and AI pathology. And the checkpoint-refractory problem is being attacked from multiple mechanistic angles simultaneously: bispecific redesign, intratumoral reprogramming, and ADC-mediated immune priming. The convergence between new drugs and new measurement is the story of this year's floor.
But the 61 first-in-human and early-phase abstracts in HNSCC are overwhelmingly single-agent, single-biomarker designs. The molecules are novel; the trial designs are not. Adaptive dosing, multi-arm biomarker-driven basket designs, and AI-augmented patient selection are largely absent from the HNSCC early-trial floor — even though the biomarker infrastructure to support them is being built in the same building. Of 358 HNSCC abstracts, the number that use AI as a trial-design methodology — not as a biomarker tool, but as a design tool — is vanishingly small.
For drug developers reading this floor, three actionable directions stand out. First, combination design over monotherapy: IL-1α-mediated resistance spans all EGFR-TKI generations, so any EGFR-targeting agent entering HNSCC should plan an anti-inflammatory combination arm from Phase 1 — not as a rescue after single-agent failure. Second, biomarker-matched patient selection from day one: the salivary fragmentome and AI-derived histopathology scores are now validated enough to stratify patients in early trials, yet no FIH abstract at this meeting used them as enrollment criteria. The first sponsor to embed saliva-based ctDNA monitoring into a dose-escalation protocol will have a structural advantage in both safety signal detection and response prediction. Third, HPV-negative as a design-level variable, not a subgroup analysis footnote: fourteen abstracts confirmed that HPV-negative HNSCC has distinct exhaustion biology (CXCL14 deficit, antigen-driven T-cell burnout) that demands its own therapeutic hypothesis — not the same checkpoint combination tested in the HPV-positive population with a subgroup forest plot.
That gap — between the biomarker infrastructure being built and the trial-design layer that should be using it — is where Pillar 1 works. Computational landscapes for early HNSCC trials, AI-augmented FIH scout systems, and the design-layer translation that this meeting confirmed is missing. The infrastructure exists. The clinical translation has not happened. That is the work.